
The Covid-19 pandemic has exposed and increased the accumulation of social inequalities in Seine-Saint-Denis: it aggravates the already degraded health status of the urbanized and racialized working classes [1] who live there (see "Covid-19 in Seine-Saint-Denis (1/2): When the Pandemic Entrenches Health Inequalities"). The health system, too, has played a role in the excess mortality that has affected the département’s population, due to inequalities in medico-social care that result from decades of liberalization, budgetary restrictions, and the indexing of health policies to profitability imperatives (Abecassis et al. 2019; Juven et al. 2019). The degraded state of the health system, combined with a management of the health crisis that overexposed those working on the front lines to the virus, explains why it has affected working-class residents and health professionals in Seine-Saint-Denis more than elsewhere and in different ways. [2]

© French ministry of health and solidarity, press release, April 30, 2020.
An urban health-care desert highlighted by the pandemic
Hospitals or city medicine: whatever the entry point into the health system that one considers, Seine-Saint-Denis appears to be a "medical desert", an expression that has long been associated with rural départements. The particularity of the département is that it is a urban medical desert. To continue the comparison with the Grand Est, the majority of the population of the Moselle département lives in urban areas of less than 50,000 inhabitants and in rural communes; yet Seine-Saint-Denis has fewer public hospital beds, fewer cardiologists, fewer general practitioners per 100,000 inhabitants.
Nationally, in terms of health resources and facilities, Seine-Saint-Denis is consistently ranked at the bottom and behind Moselle (Figure 2): 94th out of 100 départements for the number of public hospital beds per 100,000 inhabitants (Moselle ranks 70th); 91st in terms of medicalized beds for the over-75s (Moselle: 79th); 89th département out of 100 for the number of general practitioners per 100,000 inhabitants, with nearly one-third fewer doctors than the hexagonal average (Moselle: 77th).

© PopSanté 2020. Sources: CNOM, STATISS-DREES and Insee.
Moreover, the evolution over the last five years of the number of general practitioners per 100,000 inhabitants shows that Seine-Saint-Denis has fallen further behind the rest of the country (Figure 3).
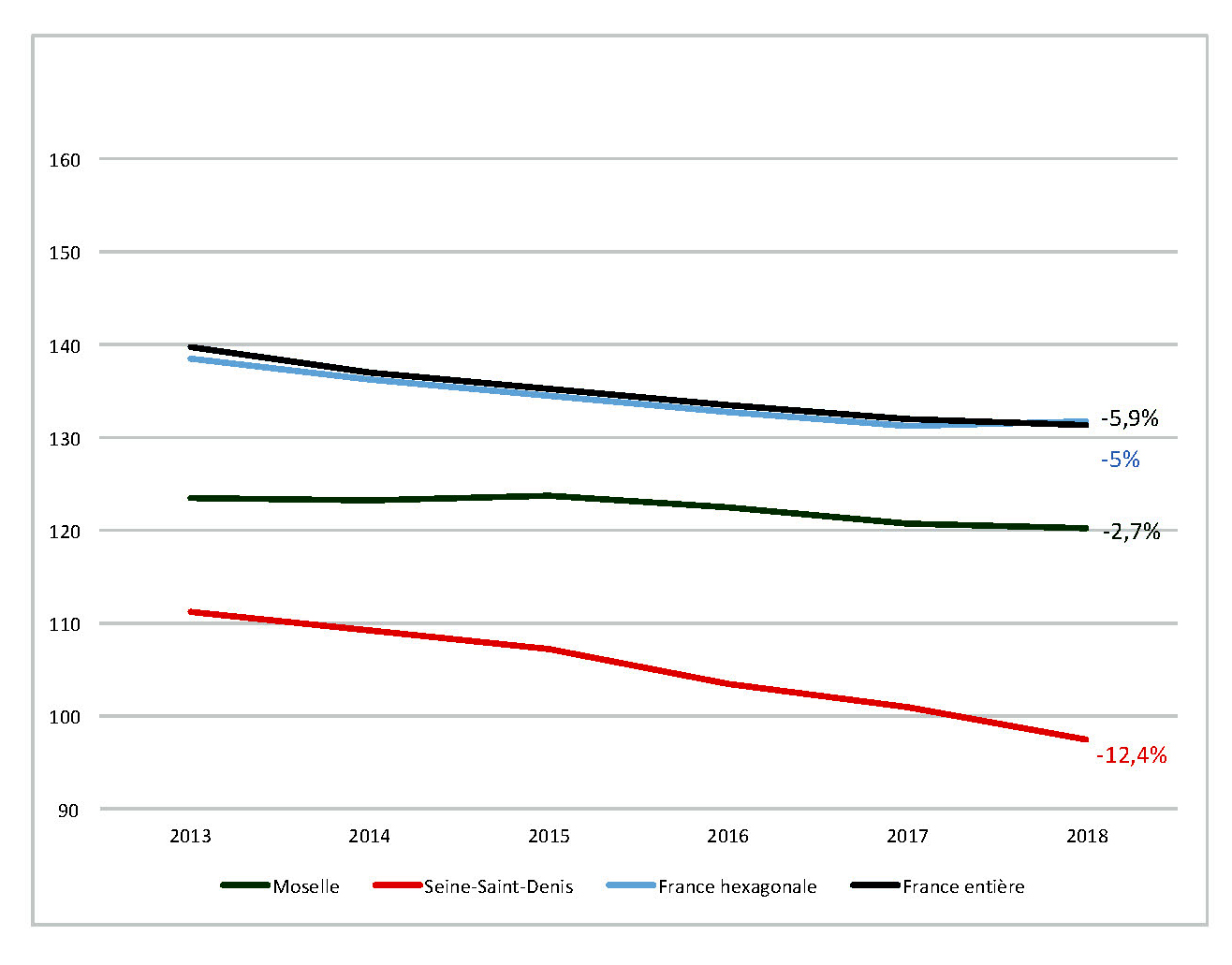
© PopSanté 2020. Sources: CNOM and Insee.
A département that always draws the short straw when it comes to health policy
In Seine-Saint-Denis more than elsewhere, the "ambulatory shift" that has structured health policies for the past fifteen years has all the hallmarks of a mirage (Juven et al. 2019, p. 41). The constant reduction in the supply of care in town medicine, combined with the département’s under-staffing of hospital beds, or even the reduction in their number as our survey in Rouvil showed between 2012 and 2016, affects the medical care of the population. The case of Seine-Saint-Denis makes it necessary to include "the supply and quality of care - that is, the way in which the healthcare system and the healthcare professions are organized" (Gelly and Pitti 2016, pp. 9-10) in the analysis of health inequalities. Patients in Sequanza-Dionysian hospitals, whose economic and social precariousness makes care more complex for medical and social professionals who may judge them as "bad" patients, are often considered "unprofitable" in a hospital economy now built on the distinction between patients who make money and patients who cost money.
The département thus has a triple handicap: fewer doctors, both general practitioners and specialists; fewer hospitals and fewer beds; and less access to and use of health care. A very high proportion of people in the département benefit from universal health coverage (which became universal health protection in 2016), which aims to enable unemployed people to benefit from social coverage, and even more from the complementary CMU, a supplementary health insurance for people on low incomes. At the beginning of 2016, 7% of the inhabitants of Seine-Saint-Denis benefited from the CMU/PUMA compared to 3.7% in Île-de-France; 14.4% from the CMU-c compared to 7.5% in Île-de-France. However, a recent study by the Défenseur des droits showed that the CMU and the Aide Médicale d’Etat for foreign patients without a residence permit caused many health care providers to refuse care (Chareyron et al., 2019). Moreover, many patients simply do not have coverage and cannot pay for a consultation; many do not have a mutual insurance company and cannot advance the medical expenses.
However, considering the département level masks significant intermunicipal disparities, particularly in terms of primary care - in particular, depending on whether the GPs are private or salaried (practicing in municipal, associative or private health centers, or in maternal and child protection centers). Rouvil appears to be less disadvantaged than the rest of the département: it has a higher density of private general practitioners (61 per 100,000 inhabitants compared to 55.1 for the département as a whole in January 2016), complemented by a greater supply of municipal and associative health care than elsewhere in the département (more than a third of general practitioners practicing in "town medicine", i.e. elsewhere than in hospitals, were salaried at the end of 2016 in municipal health centers). This specificity, linked to a local health policy whose history precedes by several decades the territorial turn of public action in health at the national level (Mariette and Pitti 2019), is not, however, representative of the communal health care offer in the whole département. Olivier Klein, mayor of Clichy-sous-Bois, testifies to this: "Working-class neighborhoods are real medical deserts, and the State must rethink local medicine and reinvent a public policy of territorial health centers. In some municipalities, there are municipal health centers, but they are expensive for the municipalities. In my town, I don’t have the means." [3] Seine-Saint-Denis is a magnifying mirror of the double movement of increasing social and territorial inequalities produced by the supposed "ambulatory shift" in health policies, so much so that "the transfer of activity from the hospital to the ambulatory translates into [...] a transfer of charges from Social Security to the territorial authorities, which partly finance medico-social care" (Juven et al. 2019, p. 47).
In Seine-Saint-Denis, waiting times to obtain a general medical appointment remain longer than elsewhere (Millien et al. 2018, p. 3), even though the needs are greater due to the health status of the populations and there are also fewer specialists. This supply of care is very poorly compensated for by the proximity of Paris, due to the price of medical consultations in the capital (Vergier 2016, p. 3). Whether private or municipal, general practitioners’ offices are therefore often overcrowded.
Medical clusters and scarcity medicine
At the height of the epidemic, these overcrowded practices were able to constitute real "medical clusters", even before the over-occupation of housing, combined with the lower proportion of teleworkers in Seine-Saint-Denis than elsewhere, increased the "family clusters", and this all the more so since the alert on the spread of Covid-19 in France was late in being launched by the government (Marichalar 2020) despite the feedback from several hospital infectious-disease departments. [4] Just as much as hospital workers, or even more so according to the first results of a national survey, [5] price for the epidemic: as of April 26, there were 34 deaths of Covid-19 caregivers in France, including almost half of general practitioners in private practice. A quarter of them were practicing in Seine-Saint-Denis. [6]
Many of the testimonies of health care workers involved in the movement to defend the public hospital for more than a year, who have had to fight against Covid-19 in Seine-Saint-Denis, are along the same lines. Yasmina Kettal, a nurse in an emergency room at one of the département’s hospitals and one of the spokespersons for the Inter-Emergency Collective, [7] thus put forward the "medicine of scarcity" that they had to practice in the hospitals of the département in this prior context of under-equipment and restrictions, cruelly highlighted by the health crisis. Christophe Prudhomme, emergency doctor at Samu 93, spokesman for the association of emergency doctors of France and member of the board of the CGT-Santé, specified: "We were the first département of Île-de-France to have no more resuscitation beds available at the peak of the epidemic. In Seine-Saint-Denis, there are fewer public services, fewer doctors and fewer hospitals. Our hospitals are in a lamentable state. " [8]
Our survey in Rouvil made it possible to measure this: the organization of the teams to deal with the epidemic was based on forms of professional commitment, which we had observed before the epidemic and which we saw particularly reactivated in the context of a health crisis, characteristic of social medicine in working-class territories, attentive to social inequalities and a "global approach" to the health of the populations (Mariette and Pitti 2016). This professional commitment is often the work of doctors whose social origins are more modest than they generally are in the medical profession and who, for many, practice medicine as a public health mission, or even reconvert forms of militant commitment into their medical practice. Without a doubt, the mobilizations for more than a year in defense of the public hospital, which started in the paramedical professions and ended up reaching the doctors, will have played a role in the capacity of the hospital teams to organize themselves to face the tidal wave of the epidemic in Seine-Saint-Denis in a context of generalized shortage of masks, gowns and tests. The first elements drawn from the survey conducted during the crisis tend to show that the links forged within and between the groups mobilized to defend the public hospital have reshuffled the cards of hierarchies, which are strong in the hospital environment, and have constituted a favourable terrain for the local reorganization of teams, which is decisive in the fight against the virus. Similarly, the "extraordinary parenthesis" [9] that the health crisis constituted in the management of the hospital, in terms of means as well as the organization of work, nourishes the contestation. The fact remains that, in Seine-Saint-Denis, this shortage has been combined with a long-standing lack of equipment and health resources, which has weighed heavily on the epidemic’s toll - to the point of making it the French département where people die of Covid younger than elsewhere.
Inhabitants’ solidarity in the face of the state’s failings
In working-class neighborhoods, long-standing forms of local solidarity and mutual aid have been reconfigured with the process of disengagement of the social state since the 1980s-1990s (Trenta 2015; Oualhaci 2017, pp. 197-316). This disengagement has gone hand in hand with the rise of the associative world in the implementation of social and health policies at the local level and the delegation of public services to associations (Cottin-Marx et al. 2017). It is this solidarity and this associative fabric - variable according to municipalities and neighborhoods - that the current crisis has activated, not "reinvented": these solidarity practices, carried by multiple associations, have been highlighted by the health crisis.
These forms of solidarity - many of which have focused on food and housing issues, in Seine-Saint-Denis as elsewhere - reveal the State’s failure to fulfill its public health mission, which has been enshrined since 1946 in the preamble to the World Health Organization’s constitution. From this point of view, promoting real equality requires offensive and proactive measures to reduce inequalities, by making "differentiation the instrument of equality" (Borgetto 2008). This also implies (re)making health a regalian mission of the State and rebuilding a public health policy [10] that is attentive to socio-spatial inequalities, i.e., neither strictly vertical nor medico-centric. Public health cannot rely solely on voluntary policies at the city level or on initiatives by committed actors. Nor can it depend on "project-based" funding and short-term local experiments (Mariette 2017; Mariette and Pitti 2019). It requires sustainable funding that is proportional to the delays to be made up. But public health also requires improving the supply of care, i.e., the provision of health infrastructure and doctors, as a priority in the 93. Otherwise, the lives of the inhabitants of Seine-Saint-Denis will continue to be worth less than elsewhere.
Bibliography
- Abecassis, P., Coutinet, N., Juven, P.-A., Vincent, F. 2019. « La santé, un business ? », in Fondation Copernic (dir.), Manuel indocile de sciences sociales. Pour des savoirs résistants, Paris : La Découverte, p. 142-150.
- Borgetto, M. 2008. « Égalité, différenciation et discrimination : ce que dit le droit », Informations sociales, n° 148, p. 8-17.
- Chareyron, S., L’Horty, Y. et Petit, P. 2019. « Les refus de soins discriminatoires : tests dans trois spécialités médicales », Études et résultats, octobre.
- Cottin-Marx, S., Hély, M., Jeannot, G. et Simonet, M. 2017. « La recomposition des relations entre l’État et les associations : désengagements et réengagements », Revue française d’administration publique, n° 163, p. 463-476.
- Gelly, M. et Pitti, L. 2016. « Une médecine de classe ? Inégalités sociales, système de santé et pratiques de soins », Agone, n° 58, p. 7-18.
- Juven, P.-A., Pierru, F., Vincent, F. 2019. La Casse du siècle. À propos des réformes de l’hôpital public, Paris : Raisons d’agir.
- Marichalar, P. 2020. « Savoir et prévoir. Première chronologie de l’émergence du Covid-19 », La Vie des idées [en ligne], 25 mars.
- Mariette, A. 2017. « Des agents locaux aux prises avec une catégorie floue d’action publique. Enquête sur la “santé publique” dans une commune populaire de la banlieue parisienne », Lien social et politiques, n° 78, p. 151-170.
- Mariette, A. et Pitti, L. 2016. « “Médecin de première ligne dans un quartier populaire”. Un généraliste en banlieue rouge des années 1960 aux années 2010 », Agone, n° 58, p. 51-76.
- Mariette, A. et Pitti, L. 2019. « Travailler en santé publique, classer des populations : reproduction ou contestation de l’ordre social ? », conférence en session semi-plénière Classer pour soigner ? Pratiques (inter)professionnelles de classement dans le monde de la santé, Congrès de l’Association française de sociologie, 29 août.
- Millien, C., Chaput, H. et Cavillon, M. 2018. « La moitié des rendez-vous sont obtenus en 2 jours chez le généraliste, en 52 jours chez l’ophtalmologiste », Études et résultats, n° 1085, octobre.
- Oualhaci, A. 2017. Se faire respecter. Ethnographie de sports virils dans des quartiers populaires en France et aux États-Unis, Rennes : PUR.
- Trenta, A. 2015. « Les pratiques associatives dans les banlieues de Paris et Buenos Aires. La comparaison de cas contrastés », Espaces et sociétés, n° 163, p. 41-55.
- Vergier, N. 2016. « Accessibilité aux professionnels de santé libéraux : des disparités géographiques variables selon les conditions tarifaires », Études et résultats, n° 970, juillet.




















