
On September 18, 1896, the first case of bubonic plague, in all likelihood spread by rats on board a boat from Hong Kong, was detected in Bombay (today Mumbai). [1] As the first Indian city to be infected, owing to the size and importance of its port, Bombay paid a heavy price for the disease, which took hold there for the best part of two decades. Up until 1914, every winter would see a resurgence of the epidemic, which would then decline in the spring, killing almost 184,000 people in a little under 20 years, out of a total estimated population of 820,000 at the start of the 1890s.
This article seeks to question the consequences of the crisis provoked by the epidemic on the social morphology of the city and on urban policy implemented by the British colonial authorities. From the 1860s through the 1880s, the authorities focused solely on what they considered to be the nerve centers of their domination: the development of the port and the construction of adminstrative buildings befitting Bombay’s status as regional capital. Did the crisis fostered by the epidemic lead them to change their priorities?
A changed view of the city
When the plague reached Bombay, a whole section of the city, inhabited by working-class populations, was still largely unknown to the authorities (Figure 1). This was the case in particular for the inner-city factory districts that, following the rapid rise of a cotton industry from the mid‑1850s, developed to the north of older neighborhoods, beyond the control of the colonial auhtorities. In a particularly revealing manner, before the cartographic survey undertaken in 1914, the British had no precise maps of these spaces. The arrival of the plague profoundly changed the way in which they considered and understood these areas.

Indeed, at the start of the epidemic, the etiology of the disease was still largely not understood by the authorities, particularly the health authorities. Two theories coexisted: the contagionist theory, which held that the human body was the primary vector, and the infectionist theory, which linked the appearance of the disease to local sanitary conditions and considered “that a place catches the infection and that any person who stops at that place runs the risk of catching the plague” (Condon 1900, p. 11). The measures advocated therefore targeted the urban space and ranged from disinfection to the destruction of the buildings deemed most unsanitary. As knowledge of Pasteur’s discoveries spread, this last theory was quickly disavowed by scientific authorities (Kidambi 2007).
However, the infectionist approach remained very present in the practice of the administrators, particularly because of the resistance to measures targeting the bodies. In March 1898, for example, an attempt to force the hospitalization of a weaver’s daughter led to a violent riot, during which two British soldiers were killed. If, under the pressure of popular mobilizations, the authorities were forced to abandon the most drastic measures, they maintained the operations concerning the building, which were the subject of a wider consensus in the population. These were an opportunity to show that they were still working to eradicate the epidemic and to reassert their shaken control over the city.
The epidemic thus gives rise to an intense production of knowledge about urban space. [2] Each resurgence of the disease gives rise to meticulous descriptions of its geographical path, as teams of administrators and volunteers relentlessly survey the streets, searching for suspected cases and entering the interiors of dwellings for the first time. While the sources of the previous period described a socially undifferentiated insalubrity, those produced during the epidemic associated it with certain populations, the popular masses, and their practices. Colonial and indigenous elites now perceived working-class neighborhoods as epidemic nests, whose immediate proximity posed a pressing danger to their health (Caru 2013, pp. 77–82).
The Bombay City Improvement Trust, or the production of a bourgeois urbanity
One of the central concerns of the authorities was the peril that the epidemic posed to the imperial economy. The international conference in Venice in 1897 threatened to quarantine ships from Bombay, while the first violent attack of the disease led to a moment of mass panic, causing nearly 400,000 people, almost half the city’s population, to flee. This was followed by a dislocation of the labor market and an almost total collapse of the city’s main industry, the textile industry. The crisis caused by the plague was an opportunity for the British authorities to question the status quo that had prevailed since the 1860s, by which they had agreed to delegate some of the prerogatives of urban management to the local property-owning classes, with the creation of the Bombay Municipal Corporation.
In 1898, the establishment of an ad hoc organization, the Bombay City Improvement Trust (BCIT), which was almost totally dominated by the British authorities, was the instrument of this return to control: while arrogating to itself a part of the resources – particularly land – of the municipal authorities, the British authorities took over the areas of urban policy that they considered essential to the defence of their interests. The agenda set out in the BCIT’s first annual report shows that solving the health crisis, while constantly put forward as a justification for the high level of expenditure envisaged, is far from being its only ambition. It also aimed to “create new streets, open up overcrowded spaces, reclaim from the sea new land for the future expansion of the city,” [3] objectives that seemed to extend the work undertaken in the preceding decades to endow Bombay with the attributes of a modern metropolis.
The Trust’s record on health policy is very poor, if not questionable. After the implementation of five operations aimed at eradicating areas declared unsanitary during the first years of its existence, the authorities, arguing that this type of intervention was too costly, abandoned them from 1909 onwards and concentrated on the implementation of major breakthroughs. The Trust was not legally obliged to rehouse the people displaced by its operations, and it displaced nearly 64,000 people, of whom only 20% were offered a rehousing solution. The remaining 80% had no other recourse than to “rush into already overcrowded localities and thereby make them even more unhealthy,” [4] further aggravating the crowded conditions that the health authorities constantly denounced as sources of epidemic danger.
If the BCIT’s action in the sanitary field was limited, to say the least, it nevertheless contributed significantly to modifying the urban and social morphology of Bombay. Its modus operandi, first of all, was based on cooperation between public intervention and private initiative which, while satisfying the colonial authorities’ concern for profitability, gave them significant control over the production of buildings. By expropriation, the Trust acquired the land necessary for the implementation of its projects, but once the road was laid out, it awarded the leases of the plots not used by the public road to the highest bidder, through an auction system. Private contractors are thus in charge of construction, provided they subscribe to precise specifications established by the BCIT concerning the size of the buildings, the species of trees to be planted along the roads, etc. The consequence of this modus operandi is that the cost of land increases sharply and serves the interests of the wealthy classes, who are the only ones able to assume such a cost, and who are thus allocated new residential and leisure spaces. The architectural standards defined thus allow the construction of posh districts, of commercial galleries sheltered under arcades. The freed up plots of land were particularly popular with leisure entrepreneurs, and were the boon of the latest urban entertainment, the cinema. Until the First World War, the main projection venues were concentrated in the area of the Sandhurst Road breakthrough. [5]
In addition, the creation of the Trust allowed the colonial authorities to take advantage of the transformations in urban growth caused by the outbreak of the disease. The epidemic contributed to a new direction in the urban expansion of the wealthier classes: people who could cover their daily transportation costs left the dense central districts to take refuge in the northern suburbs, which were still largely agricultural. By March 1898, nearly 45,000 people had settled in the northern part of the peninsula, or on the neighboring island of Salsette. From 1899, the Trust began to develop large-scale projects. On the eve of the First World War and at the end of massive expropriation campaigns, it found itself in charge of two ninths of the city’s land, [6] ensuring that the colonial authorities had a firm grip on land resources.
Building for workers: a happy by‑product of the epidemic
The Trust was also given the task, at the time of its creation, of carrying out a large-scale building program designed to house 50,000 adults over ten years. [7] The authorities even considered, at first, subsidizing these construction sites, which was totally unprecedented. The fear aroused by the popular riots and the dislocation of the labour market forced them to make this major departure from their laissez-faire policy in this area. However, the return to order and the reappearance of an abundant labour force, driven out of the countryside by the outbreak of a famine, quickly made the deficits agreed to for workers’ housing seem less necessary. As early as 1902, the Trust made a return to the logic of the market, announcing that it would henceforth restrict itself to “constructing buildings that satisfy commercial criteria, so that they may be models for the private sector to follow.” [8]
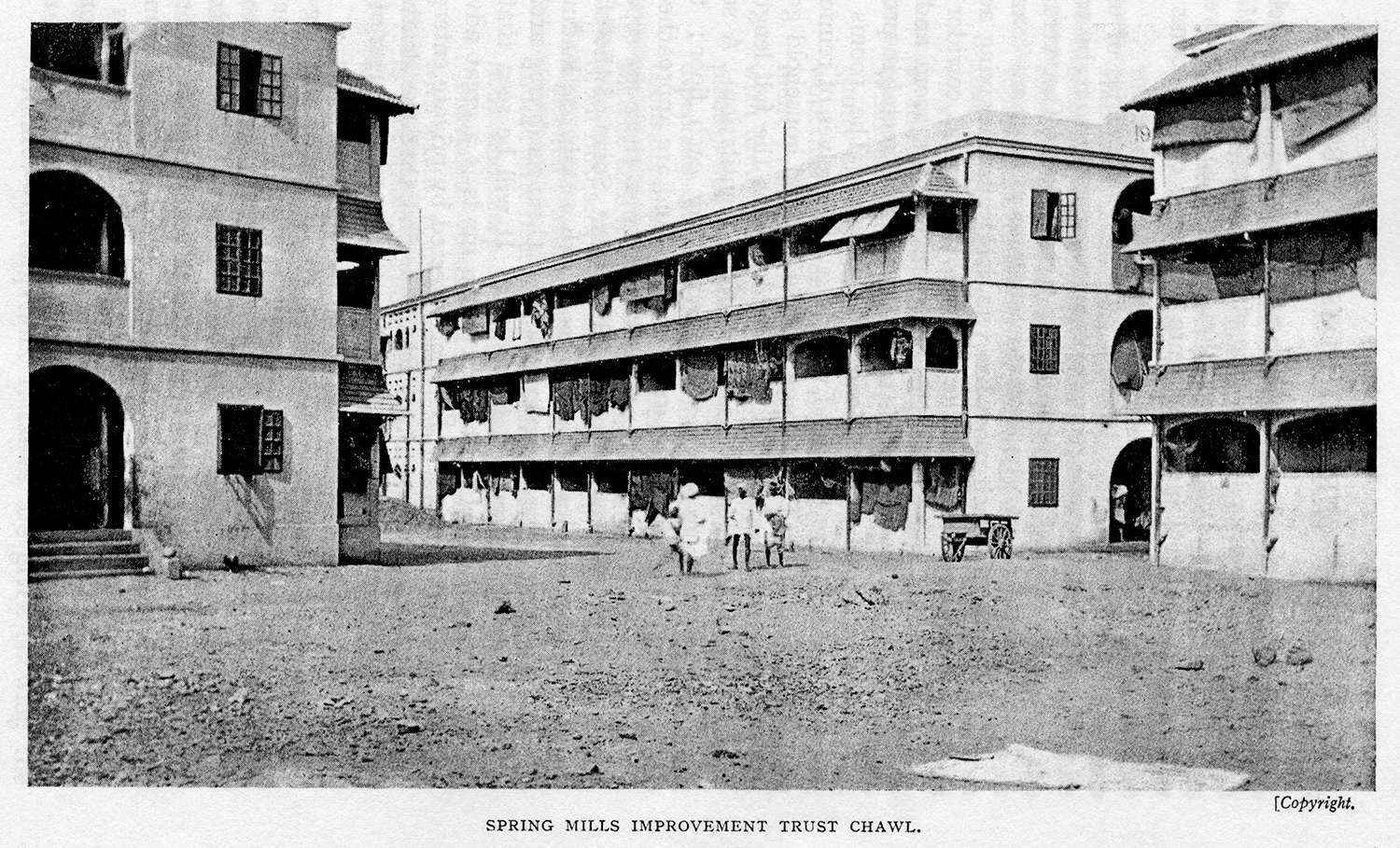
By 1918, 4,234 dwellings were built, allowing the authorities to accumulate a certain amount of expertise in the field of construction for workers. However, contrary to what was happening in England, where a real reflection on popular housing was developing, the Trust was content to make small improvements to the type of tenement building most commonly built by private owners, the chawl (Figure 2), whose tiered structure and the size of the dwellings, reduced to one room, aroused strong criticism from the health authorities. The only innovation introduced was of a technical nature with the development, during the 1910s, of a reinforced concrete structure, the use of which was still not widespread in India but on which the engineers based their hopes of significantly reducing construction costs. This conservatism can be explained by the different priorities set by the colonial and metropolitan authorities: while the latter aimed to reform the working classes through housing, in the colony, the ambition did not go beyond housing the greatest number at the lowest cost (Caru 2013, p. 144–156).
Source: A. R. Burnett-Hurst, Labour and Housing in Bombay: A Study in the Economic Conditions of the Wage-Earning Classes in Bombay, London, P. S. King & Son, 1925, pp. 25–26.
The alarming social consequences of the plague thus led the authorities to acquire a legal and technical repertoire on housing for the working classes. This accumulated experience proved invaluable when, in the aftermath of the First World War, textile workers and other workers led the first general strike movements, provoking fear in the authorities. Anxious not to alienate the support of the influential industrial employers, while the nationalist movement was gaining momentum, the authorities chose to buy social peace by responding to the housing issue, rather than supporting the workers’ wage demands. They promised a program to build 50,000 homes.
Once the urgency generated by the first waves had dissipated, the epidemic did not therefore help to modify the logic underlying the urban fabric, even though it had real consequences for the social morphology of the city. With the BCIT, the authorities acquired a formidable tool for transforming urban planning, the main driving force of which was land speculation. The Trust’s operations, with the exception of the few buildings constructed to rehouse the displaced, have exclusively benefited the most affluent: landlords who have been handsomely compensated for the expropriation of their insalubrious buildings; those who, owning cheap housing, have taken advantage of the influx of displaced populations to increase their rents; but, above all, the city’s most affluent classes, who have been gratified with new residential and leisure spaces, taking on all the attributes of the new bourgeois urban modernity.
Bibliography
- Barles, S. 1999. La Ville délétère. Médecins et ingénieurs dans l’espace urbain, XVIIIe-XIXe siècles, Seyssel: Champ Vallon.
- Caru, V. 2013. Des toits sur la grève. Le logement des travailleurs et la question sociale, Bombay (1850‑1950), Paris: Armand Colin.
- Condon, J. K. 1900. The Bombay Plague. Being A History of the Progress of Plague in the Bombay Presidency from September 1896 to June 1899, Bombay: Education Society Steam Press.
- Goerg, O. 1997. Pouvoir colonial, municipalités et espaces urbains. Conakry et Freetown, des années 1880 à 1914, Paris: L’Harmattan, vol. 2, “Urbanisme et hygiénisme”.
- Kidambi, P. 2007. The Making of an Indian Metropolis: Colonial Governance and Public Culture in Bombay, 1890–1920, Aldershot: Ashgate.
- Sarkar, A. 2018. Trouble at the Mill. Factory Law and the Emergence of the Labour Question in Late Nineteenth-Century Bombay, New Delhi: Oxford University Press.




















